
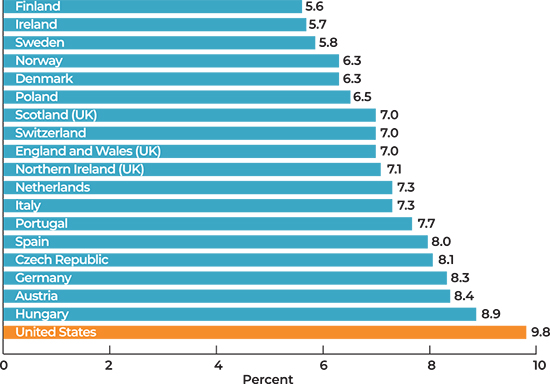
Health at birth is widely known to measure how well a society is doing,1 and birth outcomes go well beyond capturing individual behaviors. Sensitive to many stressors—including changes in the economy,2 acute crises such as 9/11,3 and worries about interpersonal racism4—birth outcomes are a reflection of how well we are doing as a country. And unfortunately, we are doing poorly relative to comparable countries, even prior to the current crisis related to COVID-19. Preterm birth (i.e. being born at less than 37 weeks of gestation) in the U.S. is much higher than in other developed countries (Figure 1),5 with one in ten babies in the U.S. born early in 2018.6
Percentage of preterm births: United States and selected European countries, 2010.
Birth outcomes matter for a thriving labor force and economy
Birth outcomes have important implications for our economy. Preterm birth costs our country an estimated $26 billion a year (in 2007 dollars).7 These costs include medical care, early intervention and special education services, as well as lost household and labor market productivity. From a human capital perspective, the opportunity costs of poor birth outcomes to our economy are high: infants born preterm are not only at higher risk for life-threatening and costly complications in their first days, but also a range of health and educational problems over their life course. When they grow up, people who were born early have lower educational attainment, employment outcomes, and incomes on average.8
Alarming and significant racial/ethnic disparities in preterm birth have persisted over decades (Figure 2). In 2018, preterm birth for Black people (14.3%) and Hispanic people (9.7%) was higher than for White people (9.0%). While estimates on preterm birth for Native Americans, Native Hawaiians, and Pacific Islanders in the U.S. are not available for the same time period, recent data on infant mortality indicate poor birth outcomes among these groups as well.9
Figure 2. Alarming Racial Disparities in Preterm Birth have Persisted Over Decades
Preterm birth rates, by race and Hispanic origin of mother: United States 1990–2013.

The opportunity costs of these racial disparities have implications for our economy as well. People of color are projected to become the majority of the U.S. labor force in the coming decades.10 Overlooking and undervaluing the potential of people of color limits the capacity of our economy.
Understanding structural inequities across the life course
While the causes of preterm birth are still largely enigmatic, a growing body of literature points to the conditions in the places where people live—especially during critical time periods of development. The places where people live during pregnancy and early childhood shape their lifelong health and even birth outcomes in the subsequent generation. The field of community development is acutely aware that place matters, and that the distribution of resources that promote health and well-being is shaped by policies and practices over time. However, what is becoming increasingly clear is that place matters especially during critical time periods, and that place has a long term impact—over lifetimes and through generations.
In a recent paper published in the American Journal of Epidemiology, my coauthors and I find further evidence to support this approach, in particular highlighting the role of structural factors in neighborhoods. We employed a measure called the Index of Concentration at the Extremes (ICE) to assess the impact of separate and combined racial/ethnic and economic segregation across the spectrum of privilege and disadvantage in neighborhoods. Developed by sociologist Douglas Massey, three ICE measures approximate three critical dimensions of privilege:
- ICE-income focuses on economic privilege by assessing neighborhood concentrations of affluent and poor residents.
- ICE-race/ethnicity centers on racial/ethnic segregation by assessing concentrations of White and Black residents (representing extreme categories of racial privilege and disadvantage in the United States).
- ICE-income+race/ethnicity represents the combination of racial and economic neighborhood privilege (White privilege and affluence versus Black racial disadvantage and economic deprivation).
This is the first study we know of that looks at ICE measures in relation to birth outcomes for two separate time periods—both early childhood and adulthood. In our analysis of 379,794 California-born mother-infant pairs, we found that the risk of preterm delivery increased as the level of privilege in a mother’s neighborhood declined, both in her neighborhood as a young child and in her neighborhood as an adult. Adjusting for neighborhood conditions in both early childhood and adulthood yielded declines in Black-White and Hispanic-White disparities in preterm delivery. These findings suggest that early childhood and adulthood neighborhood privilege each play an independent role in persistent racial disparities.
Structural measures of economic and racial segregation may be particularly important given that neighborhood disinvestment in the U.S. is a racialized phenomenon, the product of well-documented patterns of institutional discrimination across decades.11 As is well-known in the field of community development, highway funds, homeownership subsidies, and business tax incentives drew people to the suburbs starting in the 1950s. However, discriminatory institutional practices such as redlining, racially restrictive covenants, and blockbusting excluded people of color from participating in this new American symbol of prosperity and the wealth-building opportunities it offered. At the same time, manufacturing began to leave the central city for the suburbs, other regions, and eventually overseas, resulting in the patterns of economic and racial/ethnic segregation we see today. Today, targeting of discriminatory financial practices to low-income and minority communities persists—including higher cost car insurance, payday loans, and subprime loans,12—furthering conditions of concentrated neighborhood deprivation.
Babies are not blank slates
This research adds to previous literature on intergenerational health and gives support to what I call the Structural Inequities Life Course Model (Figure 3). In this framework, the experiences and behaviors of individuals over their life course are shaped by the context in which they lived: their home as a child, the street on which they played, the neighborhood in which they grew up, the policies that allowed them to live there, and the systems of privilege and oppression that resulted in policies and practices that shaped neighborhoods and the opportunities therein. Our study adds to growing evidence indicating that these factors shape the health of the next generation. From this view, babies are not blank slates. They have our history in their biology.

Broadening the framework of how we think about health and developing approaches to interrupt cycles of intergenerational inequities is essential to our future labor force and to our economy on the whole. Many approaches demonstrate promise to reduce neighborhood disadvantage and support good health in the places in which people live, work, and grow. This includes work to create healthy communities, promote equitable development, support communities facing gentrification and displacement, ensure financial stability during critical periods of development, and address racial equity. Crucial to undoing legacies of racial and economic segregation are cross-sector partnerships and systems change through the examination of power dynamics in communities. Finally, we must acknowledge that there is no silver bullet—that our solutions must be manifold, designed to reach multiple generations of family members, and sustained over time. Our current crisis of COVID-19 has sharpened the need for bold thinking. In this moment, we have the opportunity to envision new approaches that will enable all children to be born healthy and reach their full potential.
Acknowledgment: The author would like to thank co-authors Michelle Pearl, Deborah Karasek, Carolina Reid, Barbara Abrams, and Mahasin Mujahid.
1. In the past, preterm (being born at <37 weeks gestation) and low birth weight (weight less than 2500g at birth) were often considered together. Advances in accurately measuring gestational age have been helpful to distinguish premature parturition as a separate process from intrauterine growth restriction, which can result in small babies who are born at term. Current research favors a focus on preterm birth in recognition that the etiologies of both outcomes are not always related to each other. Preterm birth also largely drives infant mortality (i.e. a measure of infant who do not survive to their first birthday). As such, preterm birth is the focus of much recent research, including this blog post. 2. Margerison-Zilko, Claire E. 2011. “Economic Perturbations and Fetal Growth: A Multilevel Analysis of Exposure to Labor Market Insecurity During Gestation and Birth Weight for Gestational Age.” Dissertation.
3. Wolff, Mary S. 2016. “Birth Outcomes Soon After 9/11.” American Journal of Public Health 106, Nr. 10: 1724–1724. doi:10.2105/ajph.2016.303355.
4. Braveman, Paula, Katherine Heck, Susan Egerter, Tyan Parker Dominguez, Christine Rinki, Kristen S. Marchi, and Michael Curtis. “Worry about Racial Discrimination: A Missing Piece of the Puzzle of Black-White Disparities in Preterm Birth?” Edited by Kelli K. Ryckman. PLOS ONE 12, no. 10 (October 11, 2017): e0186151.
5. MacDorman, Marian F., T.J. Mathews, Ashna D. Mohangoo, Jennifer Zeitlin. 2014. “International Comparisons of Infant Mortality and Related Factors: United States and Europe, 2010.” National Vital Statistics Reports; vol 63 no 5. Hyattsville, MD: National Center for Health Statistics.
6. Martin, Joyce A., Brady E. Hamilton, Michelle J.K. Osterman, Anne K. Driscoll. 2019. “Births: Final data for 2018.” National Vital Statistics Reports; vol 68, no 13. National Center for Health Statistics.
7. Behrman, Richard E. and Adrienne Stith Butler. 2007. Preterm birth: causes, consequences, and prevention. Washington, D.C.: National Academies Press.
8. Currie, Janet and Rosemary Hyson. 1999. “Is the Impact of Health Shocks Cushioned by Socioeconomic Status? The Case of Low Birthweight.” American Economic Review 89, Nr. 2: 245–250. doi:10.1257/aer.89.2.245.; Heinonen, Kati, Johan Gunnar Eriksson, Eero Kajantie, A K Pesonen, David J. P. Barker, Clive Osmond and Katri Raikkonen. 2013. “Late-Preterm Birth and Lifetime Socioeconomic Attainments: The Helsinki Birth Cohort Study.” Pediatrics 132, Nr. 4. doi:10.1542/peds.2013-0951d.; Johnson, Rucker C and Robert F Schoeni. 2011. “The Influence of Early-Life Events on Human Capital, Health Status, and Labor Market Outcomes Over the Life Course.” The B.E. Journal of Economic Analysis & Policy 11, Nr. 3. doi:10.2202/1935-1682.2521.
9. Centers for Disease Control and Prevention. 2019. “Infant Mortality.” Last modified March 27, 2019.
10. “Data Summaries,” National Equity Atlas, accessed August 27, 2020.
11. Chaskin, Robert J. and Mark L. Joseph. 2017. Integrating the Inner City: The Promise and Perils of Mixed-Income Public Housing Transformation. Chicago: The University of Chicago Press.; Massey, Douglas S. 1990. American Apartheid: Segregation and the Making of the Underclass. American Journal of Sociology 96, Nr. 2: 329–357. doi:10.1086/229532.; Sampson, Robert J. 2013. Neighborhood Effects: The Evolution of an Idea. Essay. In: Great American City: Chicago and the Enduring Neighborhood Effect, 31–49. Chicago: University of Chicago Press.
12. Angwin, Julia, Jeff Larson, Lauren Kirchner and Surya Mattu. 2017. “Minority Neighborhoods Pay Higher Car Insurance Premiums Than White Areas With the Same Risk.” ProPublica. 5. April.; Calem, Paul S., Jonathan E. Hershaff and Susan M. Wachter. 2004. “Neighborhood Patterns of Subprime Lending: Evidence from Disparate Cities.” Housing Policy Debate 15, Nr. 3: 603–622. doi:10.1080/10511482.2004.9521515.;Faber, Jacob W. 2016. “Cashing in on Distress: The Expansion of Fringe Financial Institutions During the Great Recession.” Urban Affairs Review 54, Nr. 4: 663–696. doi:10.1177/1078087416684037.; Hwang, Jackelyn, Michael Hankinson and Kreg S. Brown. 2014. “Racial and Spatial Targeting: Segregation and Subprime Lending within and across Metropolitan Areas.” Social Forces 93, Nr. 3: 1081–1108. doi:10.1093/sf/sou099.; Ong, Paul M. and Michael A. Stoll. 2007. “Redlining or Risk? A Spatial Analysis of Auto Insurance Rates in Los Angeles.” Journal of Policy Analysis and Management 26, Nr. 4: 811–830. doi:10.1002/pam.20287.; Rugh, Jacob S., Len Albright and Douglas S. Massey. 2015. “Race, Space, and Cumulative Disadvantage: A Case Study of the Subprime Lending Collapse.” Social Problems 62, Nr. 2: 186–218. doi:10.1093/socpro/spv002.
The views expressed here do not necessarily reflect the views of the management of the Federal Reserve Bank of San Francisco or of the Board of Governors of the Federal Reserve System.